A 12 year-old female with no PMHx presents to the pediatric ED with acute-onset crampy and sharp left-sided pelvic pain. The pain started 3-4 hours earlier, associated with nausea but no vomiting or diarrhea.
VS: HR 102, BP 110/86, T: 99.4
You note a non-toxic appearing girl in moderate distress due to pain, with mild left pelvic tenderness to palpation but without peritoneal signs.
The rest of the exam is unremarkable.
You obtain a pelvic US which reveals the following findings:
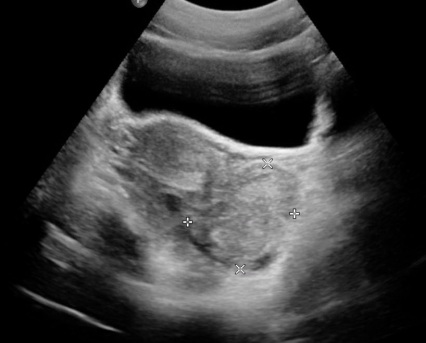
Left Adnexa.
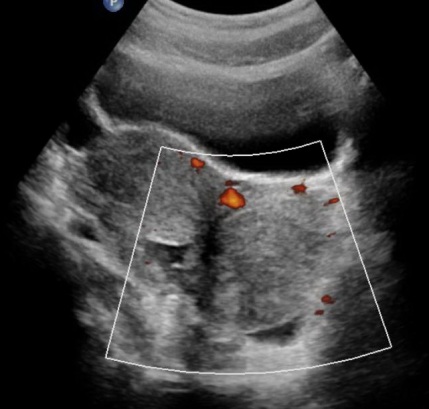
Left Adnexa
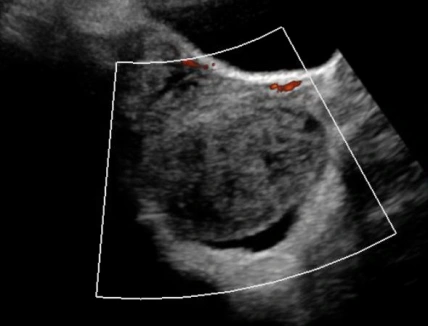
Left Adnexa
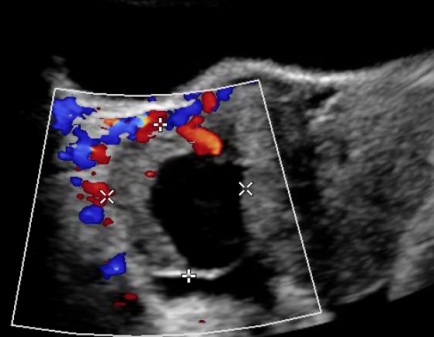
Right Adnexa for comparison
Questions:
1)What is your differential diagnosis for acute abdominal pain in the pediatric female patient?A good way of organizing the differential diagnosis for abdominal pain in the pediatric female is by system; for example:
GI: Appendicitis, cholecystitis, gastroenteritis, mesenteric adenitis, small bowel obstruction, intussusception, pancreatitis, colitis.
GU: UTI/cystitis, renal stones.
GYN: Ovarian/adnexal torsion, tubo-ovarian abscess, PID, ovarian cysts, ectopic pregnancy in the sexually active adolescent female, mittelschmerz.
MSK/abdominal wall: Spasm, hematoma, strain
2)Based on the history and physical exam for the pediatric female patient, what work up, if any, would you consider in terms of labs, imaging, and consultations?
A pelvic ultrasound is key in diagnosing pathology of the adnexa, appendix, and for identifying intussusception. The most important lab test for anyone who even has a chance of being pregnant is a pregnancy test. Other labs that are frequently ordered, although their utility is highly questionable are CBC to identify leukocytosis and inflammatory markers such as CRP. These are, however, non-specific tests.
3)Given the history, physical exam, and ultrasound findings in this patient, what is the most likely diagnosis?
This patient demonstrated decreased blood flow to the left ovary and was later found in the OR to have a necrotic left ovary which was subsequently removed.
4)What is the ED management?
ray
Latest posts by ray (see all)
- Temper Tantrums Gone Wrong – Boxer’s Fracture - March 4, 2017
- More than just a fracture! - December 21, 2016
- ST Elevation in aVR – The Widow Maker - November 10, 2016



0 Comments